 )
)������ ��
�������ڡ�ҽ��Ȧ����ʶ����վ��APP���罻ý���˺ŵij������� >>
�������ܴ��ڻ��ڷ���ĸ����㷨�������临�����븴���ԣ����������Ȼ��һ��������ս�Ե��������о��߲��á��۽���ʽ��graduated approach���������ܷ��࣬�Ӷ����˽�����ǵļ�����ͬʱ��������Ƥ֬����ֲ¡��Ч���ã��ɽ��ܶȸߡ�����ϵͳ�Բ����ܹ�ʵ�ֿ��ظ�����һ���ԣ������ʵͣ�����������ȸߡ�
����
�������������Ȳ���
����
������������������������
����
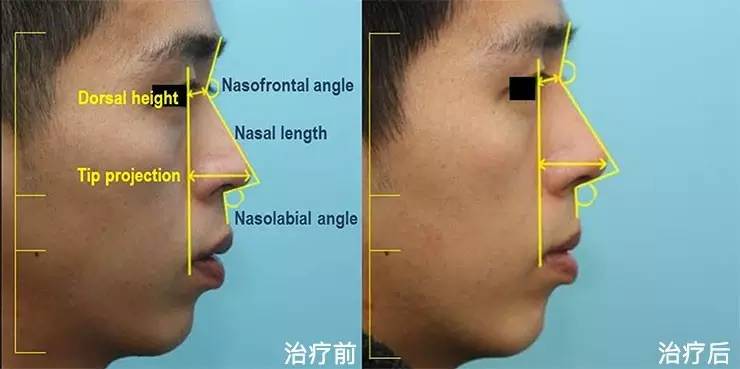
�����и���Ϲ̶�����ʾ��ͼ������ͼ��
����
��������չʾ
������������
����Dermofat was harvested under local anesthesia from the paracoccygeal area. Open rhinoplasty was performed under general anesthesia. The preoperative design was made with gentian violet at the midline from the glabella to the nasal tip, the dorsal line, the virtual portion of the anterior wedge resection and unilateral osteotomy, and the shape of the upper and lower cartilages. The stair-step incision of the transcolumellar with infracartilaginous extensions was performed at the narrowest part of the columella with no. 11 and no. 15 blades. Fine dissecting Metzenbaum scissors were used to dissect the nasal skin in a supraperichondrial plane, starting from the columellar incision. Dissection was carried out at the lateral crus and the middle crus, continuing superiorly up to the glabellar area, making a pocket for augmentation with dermofat.
����After external exposure of the upper lateral cartilage and septum, the submucoperichondrial dissection was performed using a Joseph elevator, beginning at the anterior septal angle.Bilateralmucoperichondrial tunnels were dissected deep to the upper lateral cartilages, and the upper lateral cartilages were separated from the dorsal septum.
����To correct the deviated bony framework, an anterior wedge resection in a triangular pattern was performed on the impacted side (depressed side) using a thin reciprocating saw. The first osteotomy for anterior wedge resection proceeded from the caudal edge of the impacted side just lateral to the deviated septum. The second osteotomy was performed along the ideal midline of the impacted side, usually 2 to 3 mm lateral from the first osteotomy site. After completing a triangular pattern osteotomy, a wedge segment was removed. The third (lateral) osteotomy was performed at the pyriform aperture while preserving the caudal aspect of the frontal process of the maxilla, thereby preventing collapse of the internal nasal valve.1 It continued to the level of the medial canthus superiorly and then into the oblique medially. The lateral osteotomy was not connected to the line of wedge resection, preserving the remnant bony portion. A greenstick out and in fracture of the deviated side that pivoted on the remnant bony portion was performed to reposition the deviated bone segment in the midline. The movable deviated portion of the nasal bone, together with the deviated septum, was repositioned and secured to the stable impacted portion of the nasal bone by using a 0.4-mm wire. The wire knot was located between the nasal bone and the mucoperiosteum, so that it would not to be palpable from the outer side of the skin in the longterm follow-up.
����Septal cartilage harvestwas performed preserving a 10-mmwide dorsal and a caudal L-strut. Once the septal cartilage has been removed, any remaining septal deviations of the perpendicular plate of the ethmoid or vomer can be osteotomized to remove these potential sites of interference with nasal airflow. If there is a persistent caudal septal deviation, the caudal portion of the L-strut was disarticulated from the anterior nasal spine and maxillary crest. The degree of vertical excess is assessed, and excised to be returned to the midline. The remaining caudal septum was sutured back with 3-0 nylon to the periosteum of the nasal spine.
����Harvested septal cartilage was trimmed for an adequate autologous graft. Extension grafts were mainly used to control the projection and support the tip. A fixed columellar strut was sutured to the medial crura for stabilization, tomaintain tip support, to increase tip projection, and to aid in shaping the columellar-lobular angle. Spreader grafts, onlay tip grafts, and columellar struts were used when needed.
����After the cartilaginous skeleton was sutured securely into the proper position, augmentation with dermofat was performed to correct the low dorsal height and tip projection characteristic of the Asian nose.
����Dissection for the pocket was carried out in the supraperiosteal plane up to the point of the glabella. Dermofat was sculpted to the desired size and shape and was inserted into the prepared pocket. To place the graft securely in its position, a bolster suture was performed using 3-0 blue nylon. The cranial side of the graft was fixed at the glabellar area and the caudal side of the graft was fixed at the supratip area or the columellar area according to the amount of tip projection required.
����The skin and soft tissue envelope were carefully redraped over the nasal skeleton and sutured in place with 6-0 nylon and 5-0 Vicryl sutures. A silicone sheet was placed around the nasal septum and quilt suture was performed to prevent the formation of a hematoma. Merocel (Medtronic Xomed, Jacksonville, FL) was then inserted into both the nostrils and irrigated with saline to cause inflation. A Joseph dressing was applied on the nose to secure the graft in place. Merocel packing was removed after postoperative day 5. The bolster sutures that had been placed over the nasal skin with a dermal graft were removed on postoperative day 5. Patients were instructed to keep their head elevated while they were in bed during rest and sleep for at least the first 48 hours after surgery. Any physical activity was strictly prohibited for the first 4 weeks after surgery. Intravenous postoperative antibiotics were given for 5 days.































����˵�������а�